近年来,多个大型随机对照试验均显示血小板监测评估抗血小板治疗预后的阴性结果,同时2017年ESC的DAPT指南已将血小板监测降级为III类推荐。那么,这种个体化抗血小板治疗方案到底还要继续应用吗?西班牙时间8月27日下午,ESC 2017年会上随着TROPICAL-ACS研究结果的公布再次引发热议,对此,在回顾血小板监测相关研究的同时,一起来听听ACTION研究小组Gilles Montalescot教授的建议和展望。
最后一个大型个体化抗血小板治疗随机对照研究:TROPICAL-ACS
ESC 2017年会上来自德国慕尼黑路德维希-马克西米兰大学心内科的Dirk SIBBING教授,代表TROPICAL-ACS研究组对研究结果进行了汇报。
TROPICAL-ACS研究[1]是一项欧洲多中心随机对照研究,入选人群为来自33个欧洲中心(奥地利2、波兰4、匈牙利7、德国20)的急性冠脉综合征并成功实施经皮介入治疗的患者。全部患者随机分配至对照组(无血小板功能监测、应用普拉格雷12个月)和个体化治疗组(根据Multiplate analyzer血小板监测进行降级治疗、短期应用普拉格雷后降级为氯吡格雷)。主要终点为1年的全因心血管死亡、心肌梗死、非致死性卒中以及出血学术研究会(BARC)定义的≥2级出血(净临床终点NACE)。
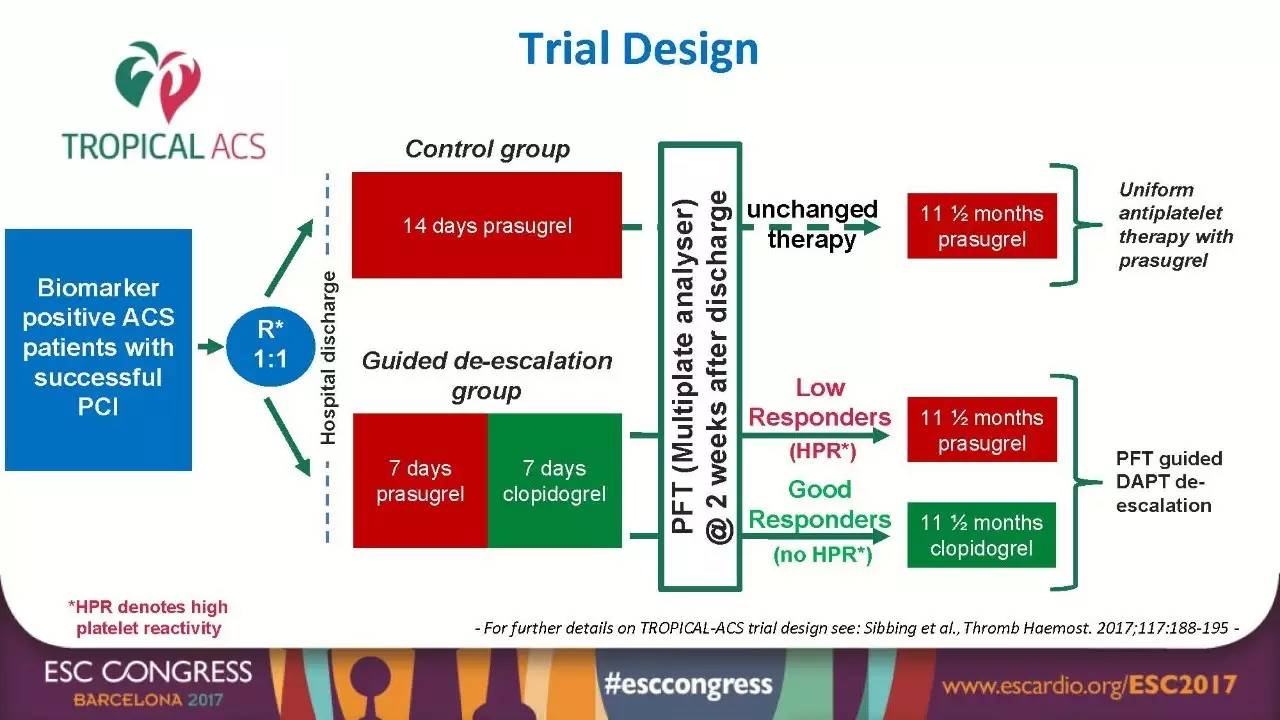
图1
研究结果显示:随访1年时,个体化组和对照组主要终点事件无优效性差异(7.3% VS 9.0%,非劣效性P=0.0004,优效性P=0.1202)。同时,随着随访时间延长,两组NACE事件小幅增加,但仍无显著差异。此外,从主要研究终点的单一事件而言,个体化组与对照组在全因心血管死亡、心肌梗死、非致死性卒中(HR 0.77,95%CI:0.48~1.21,非劣效性P=0.0115)和BARC≥2级出血(HR 0.82,95%CI:0.59~1.13,P=0.2257)亦未见明显差异。
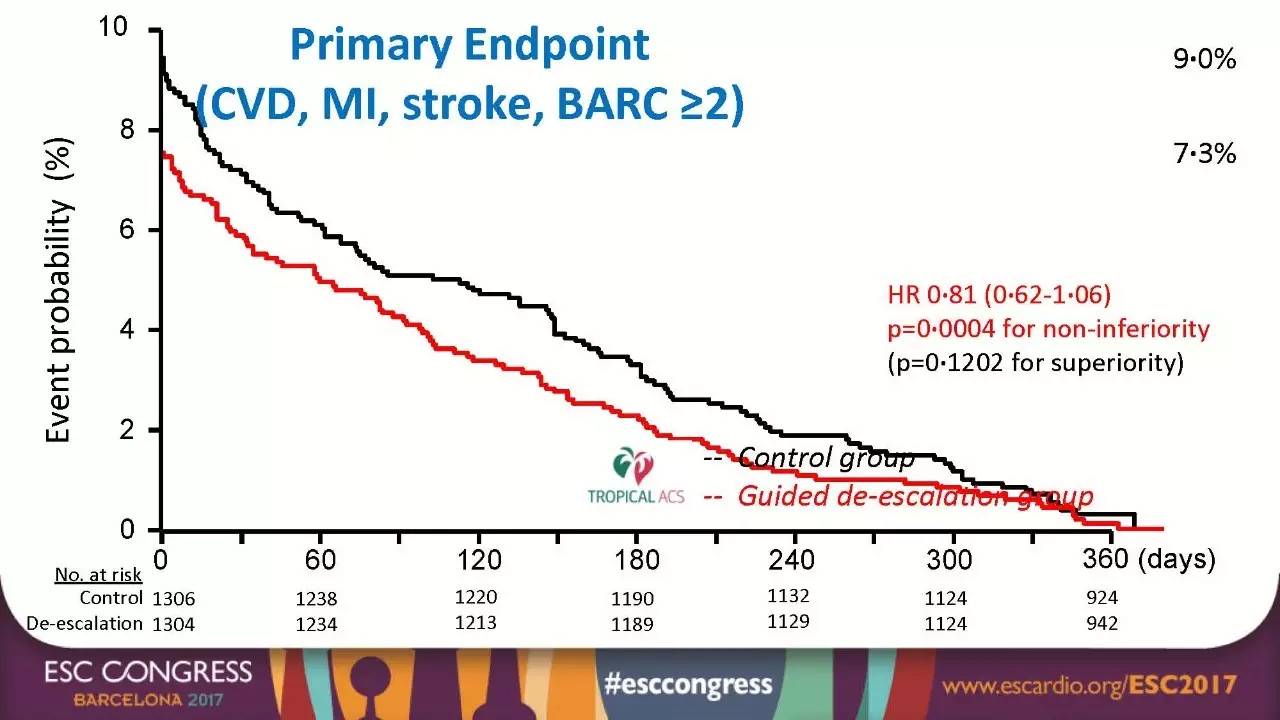
图2
为什么我们要进行个体化抗血小板治疗?
既往研究显示,血小板反应性是冠心病缺血和出血事件的强预测因素[2,3],但因人种、基因、并发症等情况存在极大的个体差异[4,5]。然而,一个合理的血小板反应性,是降低缺血和出血事件的关键,也是改善患者预后的靶点。因此,1960年开始人们应用光学比浊法(LTA)进行血小板功能检测,随后又出现流式细胞仪等多种检测方法。可惜的是,这些方法都只能在实验室进行、设备昂贵、检测方法复杂且人员资质要求高,无法广泛应用于临床。二十世纪床旁血小板功能检测技术的问世,给我们带来动态监测血小板反应性、调整抗血小板治疗方案、进行个体化抗血小板治疗的可能[6]。近十余年间,世界各国研究者们为了改善冠心病患者的临床预后,也进行了大量的相关研究。
近年相关研究的结果
起初,多项研究确定了高血小板反应性(HTPR)与缺血事件的关联[7,8]。ADAPT-DES[9~11]等研究证实了低反应者的高血栓风险和高反应者的高出血风险。同时,观察性研究的阳性结果给予了研究者极大的鼓舞。那么,既然HTPR与临床预后相关,如果对HTPR患者进行抗血小板药物调整,是否就会带来更好的预后呢?
基于此,TRIGGER-PCI[12]和MATTIS[13]研究分别将低反应者的氯吡格雷改为普拉格雷或替格瑞洛(强效新型P2Y12受体拮抗剂),而GRAVITAS[4]研究尝试了在HTPR患者中应用氯吡格雷的强化方案。这些研究发现强化抗血小板方案仅带来了HTPR的减少,但患者预后并无差异。
随后,ACTION研究小组设计了首个根据血小板监测进行个体化抗血小板治疗的大型随机对照研究——ARCTIC研究[14]。共纳入2440例冠心病患者并随机分入个体化治疗组或常规治疗组,应用VerifyNow进行血小板监测并调整用药,结果并未发现两组之间预后的差异。ARCTIC研究阴性结果被归因于试验中过少的高危患者以及应用大量的强效抗血小板药物(普拉格雷)。因此,ACTION研究小组又针对急性冠脉综合征老年患者设计了ANTARCTIC研究[15],最终个体化抗血小板治疗方案在更高危的人群中也得到了阴性的结果。
同时,2017年发表的TROPICAL-ACS研究,应用其他血小板功能监测来进行个体化抗血小板降级治疗的方案,同样无优效性推荐。
血小板监测评估抗血小板治疗还有未来吗?
多个大型随机对照试验的阴性结果,导致我们对血小板监测意义的质疑。同时,2017年ESC的DAPT指南已将血小板监测降级为III类推荐,并不做常规应用推荐。那么,到底还需要继续应用吗?为此,我们采访了来自ACTION研究小组主持ARCTIC和ANTARCTIC研究的Gilles Montalescot教授。Gilles Montalescot教授对血小板监测的未来,指出以下几点:
1.虽然床旁血小板功能监测对我们理解和认识血小板反应性有巨大的意义,但目前试验的阴性结果并不支持常规使用血小板监测来评估预后。
2.其仍在抗血小板药物的药代动力学研究中处于主导地位[16~18]。
3.可以用来监测患者抗血小板药物的依从性,尤其在出现支架内血栓的患者中更有意义[8]。
4.推荐应用于冠状动脉搭桥术(CABG)围术期的血小板功能监测,控制范围20AUC<ASPI检测≤30AUC和19AUC<ADP检测≤46AUC[19-21]。
5.目前,有大量关于脑血管或外周血管的相关研究,在这些同样需要抗血小板治疗的人群中,其意义需要进一步的探讨。

图3
Gilles Montalescot教授总结道,根据目前指南,并不推荐常规应用血小板监测进行个体化治疗。但是,其仍有一定应用空间,如药代动力学研究、药物依从性监测以及CABG围术期监测。并且,随着技术的进步,在神经科、血管科可能会有更大的发展。
参考文献:
[1]Sibbing D, Aradi D, Jacobshagen C, Gross L, Trenk D, Geisler T, et al. A randomised trial on platelet function-guided de-escalation of antiplatelet treatment in acs patients undergoing PCI. Rationale and design of the testing responsiveness to platelet inhibition on chronic antiplatelet treatment for acute coronary syndromes (TROPICAL-ACS) trial. Thrombosis and haemostasis. 2017;117:188-195.
[2]Komosa A, Siller-Matula JM, Lesiak M, Michalak M, Kowal J, Maczynski M, et al. Association between high on-treatment platelet reactivity and occurrence of cerebral ischemic events in patients undergoing percutaneous coronary intervention. Thrombosis research. 2016;138:49-54.
[3]Sabouret P, Rushton-Smith SK, Kerneis M, Silvain J, Collet JP, Montalescot G. Dual antiplatelet therapy: Optimal timing, management, and duration. European heart journal. Cardiovascular pharmacotherapy. 2015;1:198-204.
[4]Price MJ, Berger PB, Teirstein PS, Tanguay JF, Angiolillo DJ, Spriggs D, et al. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: The GRAVITAS randomized trial. Jama. 2011;305:1097-1105.
[5]Collet JP, Kerneis M, Hulot JS, O'Connor SA, Silvain J, Mansencal N,et al. Point-of-care genetic profiling and/or platelet function testing in acute coronary syndrome. Thrombosis and haemostasis. 2016;115:382-391.
[6]Paniccia R, Antonucci E, Maggini N, Miranda M, Gori AM, Marcucci R, et al. Comparison of methods for monitoring residual platelet reactivity after clopidogrel by point-of-care tests on whole blood in high-risk patients. Thrombosis and haemostasis. 2010;104:287-292.
[7]Matetzky S, Shenkman B, Guetta V, Shechter M, Beinart R, Goldenberg I, et al. Clopidogrel resistance is associated with increased risk of recurrent atherothrombotic events in patients with acute myocardial infarction. Circulation. 2004;109:3171-3175.
[8]Sibbing D, Braun S, Morath T, Mehilli J, Vogt W, Schomig A, et al. Platelet reactivity after clopidogrel treatment assessed with point-of-care analysis and early drug-eluting stent thrombosis. Journal of the American College of Cardiology. 2009;53:849-856.
[9]Stone GW, Witzenbichler B, Weisz G, Rinaldi MJ, Neumann FJ, Metzger DC,et al. Platelet reactivity and clinical outcomes after coronary artery implantation of drug-eluting stents (ADAPT-DES): A prospective multicentre registry study. Lancet. 2013;382:614-623.
[10]Kirtane AJ, Parikh PB, Stuckey TD, Xu K, Witzenbichler B, Weisz G, et al. Is there an ideal level of platelet P2Y12-receptor inhibition in patients undergoing percutaneous coronary intervention?: "Window" analysis from the ADAPT-DES study (assessment of dual antiplatelet therapy with drug-eluting stents). JACC. Cardiovascular interventions. 2015;8:1978-1987.
[11]Montalescot G, Wiviott SD, Braunwald E, Murphy SA, Gibson CM, McCabe CH, et al. Prasugrel compared with clopidogrel in patients undergoing percutaneous coronary intervention for st-elevation myocardial infarction (TRITON-TIMI 38): Double-blind, randomised controlled trial. Lancet. 2009;373:723-731.
[12]Trenk D, Stone GW, Gawaz M, Kastrati A, Angiolillo DJ, Muller U, et al. A randomized trial of prasugrel versus clopidogrel in patients with high platelet reactivity on clopidogrel after elective percutaneous coronary intervention with implantation of drug-eluting stents: Results of the TRIGGER-PCI (testing platelet reactivity in patients undergoing elective stent placement on clopidogrel to guide alternative therapy with prasugrel) study. Journal of the American College of Cardiology. 2012;59:2159-2164.
[13]Musallam A, Orvin K, Perl L, Mosseri M, Arbel Y, Roguin A, et al. Effect of modifying antiplatelet treatment to ticagrelor in high-risk coronary patients with low response to clopidogrel (MATTIS). The Canadian journal of cardiology. 2016;32:1246 e1213-1246 e1219.
[14]Collet JP, Cuisset T, Range G, Cayla G, Elhadad S, Pouillot C, et al. Bedside monitoring to adjust antiplatelet therapy for coronary stenting. N Engl J Med. 2012;367:2100-2109.
[15]Cayla G, Cuisset T, Silvain J, Leclercq F, Manzo-Silberman S, Saint-Etienne C, et al. Platelet function monitoring to adjust antiplatelet therapy in elderly patients stented for an acute coronary syndrome (ANTARCTIC): An open-label, blinded-endpoint, randomised controlled superiority trial. Lancet. 2016;388:2015-2022.
[16]Erlinge D, Gurbel PA, James S, Lindahl TL, Svensson P, Ten Berg JM, et al. Prasugrel 5 mg in the very elderly attenuates platelet inhibition but maintains noninferiority to prasugrel 10 mg in nonelderly patients: The GENERATIONS trial, a pharmacodynamic and pharmacokinetic study in stable coronary artery disease patients. Journal of the American College of Cardiology. 2013;62:577-583.
[17]Storey RF, Angiolillo DJ, Bonaca MP, Thomas MR, Judge HM, Rollini F, et al. Platelet inhibition with ticagrelor 60 mg versus 90 mg twice daily in the PEGASUS-TIMI 54 trial. Journal of the American College of Cardiology. 2016;67:1145-1154.
[18]Parodi G, Bellandi B, Valenti R, Migliorini A, Marcucci R, Carrabba N, et al. Comparison of double (360 mg) ticagrelor loading dose with standard (60 mg) prasugrel loading dose in ST-elevation myocardial infarction patients: The rapid activity of platelet inhibitor drugs (RAPID) primary PCI 2 study. American heart journal. 2014;167:909-914.
[19]O'Connor SA, Amour J, Mercadier A, Martin R, Kerneis M, Abtan J, et al. Efficacy of ex vivo autologous and in vivo platelet transfusion in the reversal of P2Y12 inhibition by clopidogrel, prasugrel, and ticagrelor: The APTITUDE study. Circulation. Cardiovascular interventions. 2015;8:e002786.
[20]Petricevic M, Milicic D, White A, Boban M, Mihaljevic MZ, Piljic D, et al. Development of a concept for a personalized approach in the perioperative antiplatelet therapy administration/discontinuation management based on multiple electrode aggregometry in patients undergoing coronary artery surgery. Journal of thrombosis and thrombolysis. 2015;40:383-391.
[21]Youn YN, Yi G, Lee S, Joo HC, Yoo KJ. Posttreatment platelet reactivity on clopidogrel is associated with the risk of adverse events after off-pump coronary artery bypass. American heart journal. 2014;167:818-825.
心在线 专业平台专家打造
编辑 潘欢丨美编 柴明霞丨制版 崔凤娟