肝损伤的治疗目的:1.明确非手术治疗肝损伤的安全性和可取性;概述肝损伤非手术治疗指征和方案;概述肝损伤的手术治疗指征和方案;
定义:肝脏损伤:
Ⅰ级:包膜撕裂,撕脱性损伤/实质性损伤<1cm深
Ⅱ级:实质性损伤1-3cm深/包膜下血肿<10cm直径外周穿透伤
Ⅲ级:实质性损伤>3cm深/包膜下血肿>10cm/中心穿透伤
Ⅳ级:大叶组织破坏性中央区血肿
五级:肝后腔静脉损伤/广泛的双叶肝组织损伤:
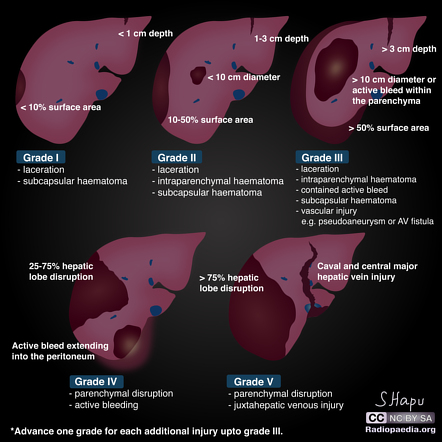
肝脏损伤AAST分级
1.肝损伤的手术和非手术治疗指征:a.当肝损伤持续出血导致生命体征不稳定或有其他损伤的可能性时,应考虑肝损伤的手术治疗。
i.腹部迅速扩张的明显不稳定患者或腹部强直。腹腔穿刺灌洗明显阳性。i i i.CT扫描为V级肝损伤。iv.CT扫描呈“漩涡”状征象,提示介入血管造影很有可能无法有效止血。V.RUQ.右上腹部高能量枪伤。
非手术治疗指征:1.血管介入造影栓塞是容易到达和控制的部位出血。
2.液体复苏后生命体征有适当的反应并逐渐好转。
3.腹部没有其他明显损伤。
4.创伤团队在血管造影室对患者进行监测。
5.在生命体征稳定的前提下,肝损伤可进行非手术治疗的其他情况。
5.1. 肝损伤在CT扫描中诊断,从1级到IV级损伤,生命体征稳定,同时:a)损伤未累及肝门。b)肝周血肿比较局限。
5.2.腹部快速超声阳性,提示腹腔积血,CT证实为单纯肝脏损伤且生命体征平稳。
2。手术处理:
2.1.立即将病人转移到手术室,准备好自动牵开器(Bookwalter);
2.1.1.消毒区域准备从下巴到大腿中部,延伸到两侧手术台边缘的腋中线;
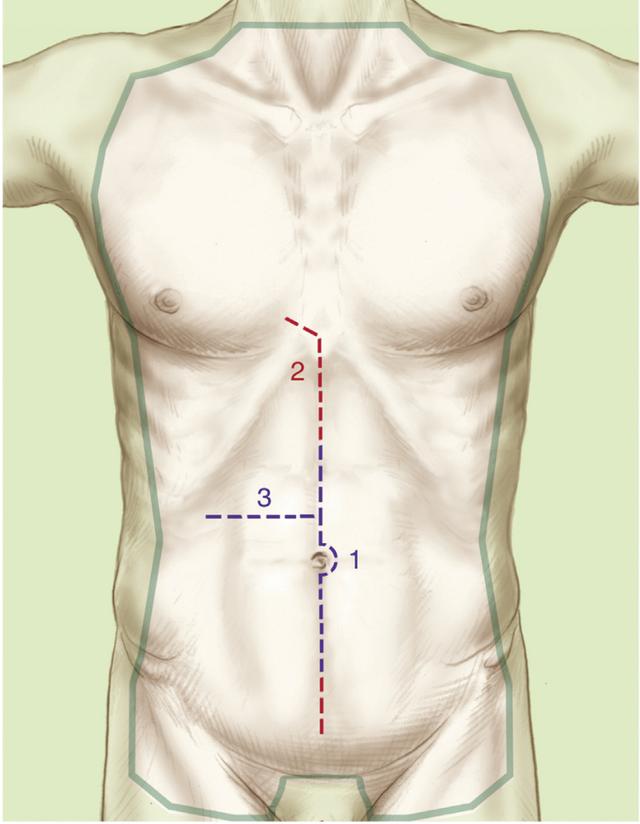
消毒区域
2.1.2.从剑突到脐下的中线长切口;2.1.3.用多个大纱垫填塞右上腹RUQ。如果出血很凶猛或病人严重低血压,考虑使用主动脉封堵器阻断主动脉!!
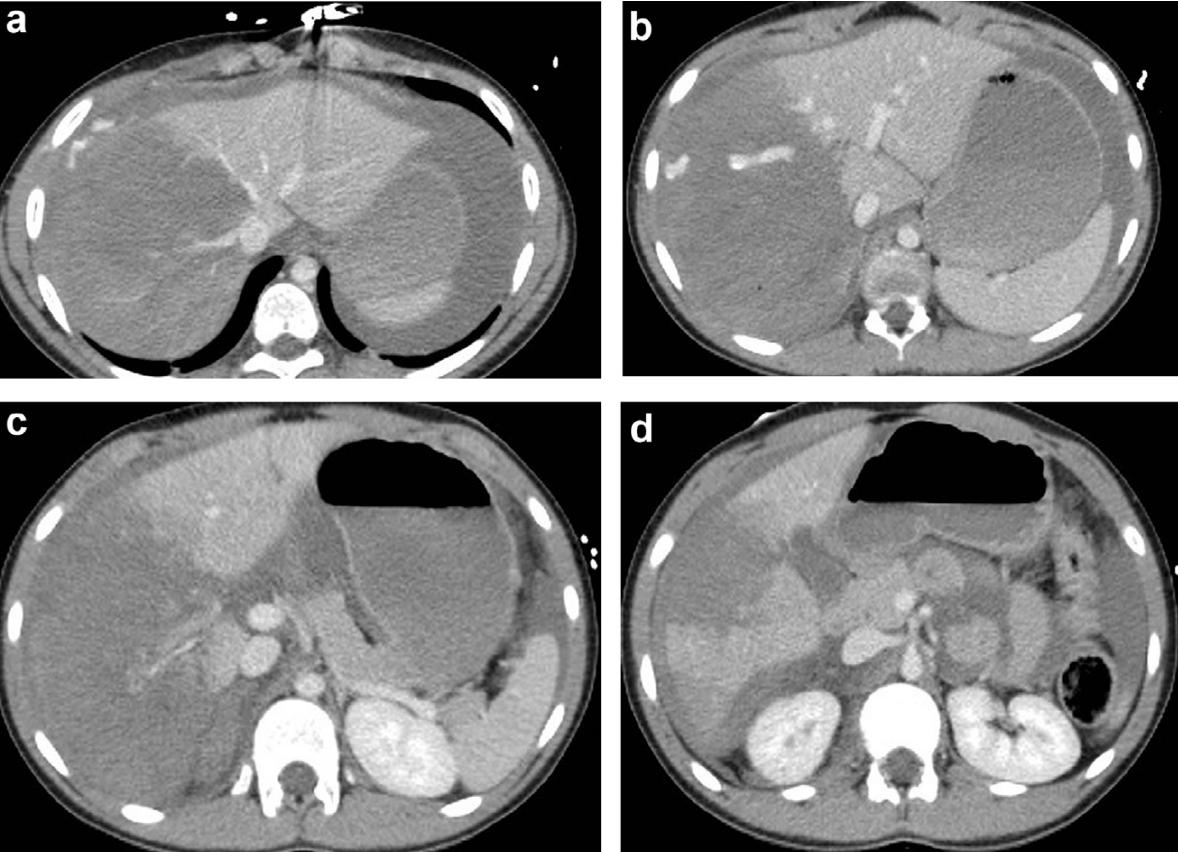
肝脏损伤4度
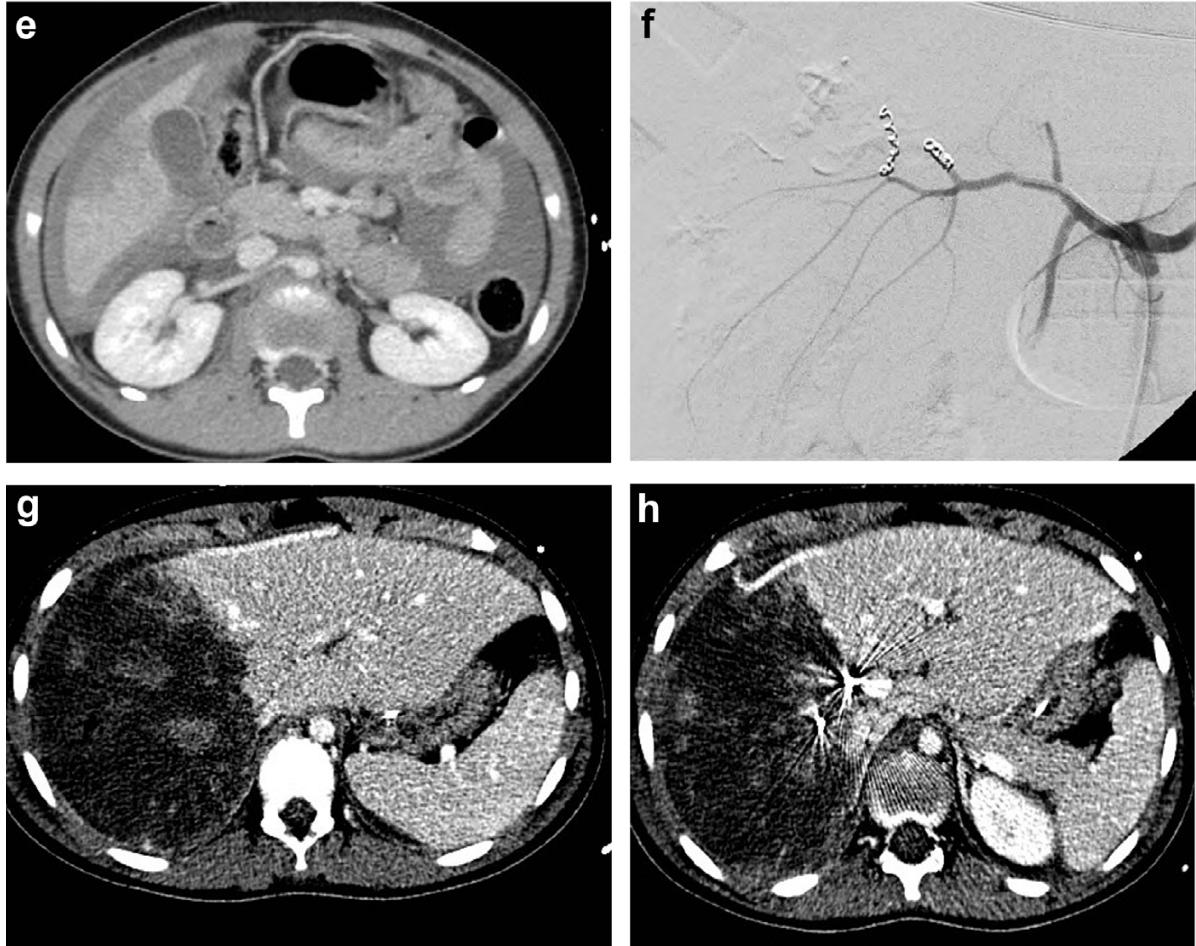
肝脏损伤介入治疗

损伤部位标记
2.2、 填塞其他象限并检查肠系膜是否出血。如果没有:
2.3.评估肝脏出血;
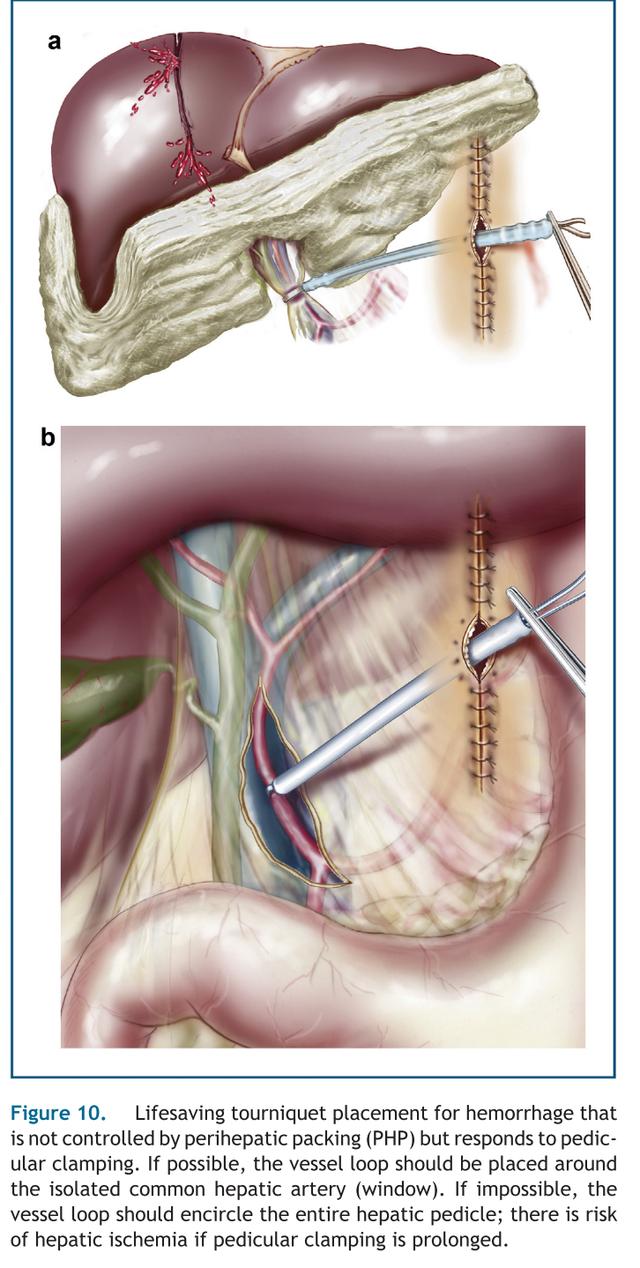
2.3.1.如果出血很凶猛,用非损伤血管钳或者Pringle手法控制肝门。
2.3.1.1如果仍然持续出血,考虑肝静脉损伤或肝后腔静脉损伤。如果有肝后静脉损伤出血:i)考虑静脉-静脉旁路。ii)考虑切除清创术以到达腔静脉和肝静脉分支。iii)考虑正中胸骨切开术以更好地控制iv)考虑填塞(见损伤控制指南)。
2.3.1.2如果出血控制:i)控制出血用缝合线结扎。ii)松开Pringle动作,用缝合线结扎控制大出血。iii)可以考虑网膜填塞。
2.3.1.3如果出血控制后,但由于凝血障碍恶化再出血,考虑临时填塞作为确定手术。
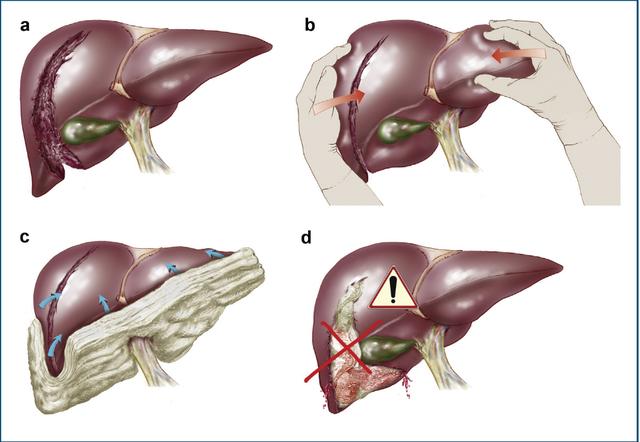
如果出血是中度程度的,但可以用填塞控制:那么可以考虑a)将肝脏适当松解:i)松解镰状韧带。ii)松解外侧冠状韧带。iii)将肝脏向内侧旋转暴露损伤部位。b)探查损伤(操作轻柔,不要加重出血)。c)用缝合方法控制出血。d)用大的可吸收缝线(0-chomic on)考虑肝脏边缘进针)。e)考虑大网膜填塞。iii.如果出血是可控的,但随后由于凝血功能而恶化,则考虑将填塞作为临时确定治疗方法。当肝出血得到控制时,探查腹部其他部位,特别注意肝门、十二指肠、胰腺和右结肠。h、 如果伤口很深,有可能出现胆汁漏和积液,则用吸引器吸干显露术野肝脏可能损伤的胆管。i.如果放置了纱布填塞,则用专门的负压吸引装置关闭腹部。j.填塞的纱布应在24-48小时内取出。准备自体输血、血液制品为该二次手术做准备。k、 如果临时填塞,建议适当使用抗生素预防感染治疗。
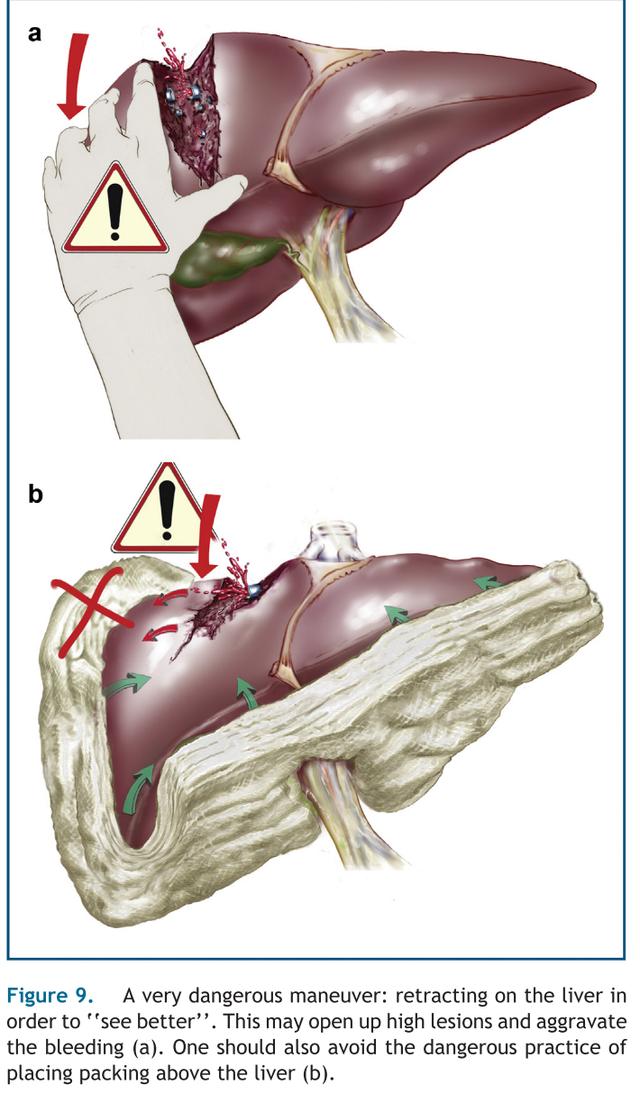
错误的手法会加重出血
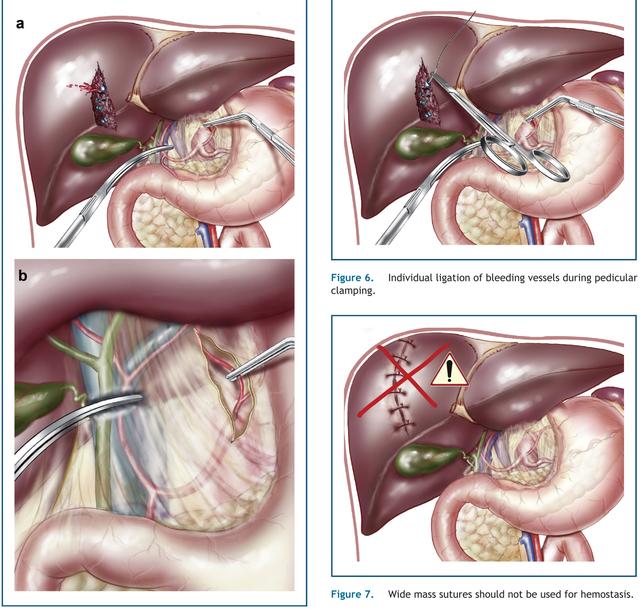
缝合注意事项
三。非手术治疗:a.将所有III-IV级肝裂伤或肝周围有明显血液(生命体征正常)的患者进行生命监测。如果红细胞压积<32%,肝脏周围有大量血液的患者送入重症监护室监护。其于患者都收入进入创伤病房。i.监测每小时的生命体征,直到生命体征正常(如脉搏<100/min)X 3.ii。卧床休息。i i i。N禁食。iv。每6小时复查一次的红细胞压积和血红蛋白,直到稳定(2%以内)X 2。
b。当红细胞压积稳定且血流动力学稳定时:i.转移到普通病房。Ii.特定饮食。Iii.每天复查红细胞压积和血红蛋白。Iv.第2天的肝酶和胆红素有助于诊断有无胆漏。如果胆红素升高,考虑HIDA扫描以排除胆漏,即卧床休息2天。一级和二级肝损伤可立即下床活动。
所有的病人都佩戴标注肝脏损伤的标志。
如果饮食稳定且耐受:a)一级和二级损伤:第1-2天出院。b) 三、四级伤害:第4天出院:一、一周内不上学。六周内不进行体育锻炼。I I I.何时进行对抗性运动:a)一级和二级:六周内禁止。b)三级、四级和五级:三个月内禁止。I V.两周后复查。V.避免饮酒。
如果:a)右上腹疼痛恶化加重b)发烧c)黄疸d)呕血,4,则迅速到急诊就诊复查。
⚠️⚠️⚠️⚠️⚠️特被要注意的关键点:a.发烧和/或黄疸-考虑胆漏。i.CT扫描可以确认肝周围有无积液。放射性核素胆道排泄检查以确认活动性胆道渗漏。i i i.经皮穿刺引流。iv.考虑ERCP支架置入和/或括约肌切开术。b.损伤后2-4周内出血-考虑胆道出血。i.CT扫描以确认肝内大损伤或血凝块。血管介入造影术以确定病变部位和原因;i i i.必要时血管造影栓塞;iv.胆道出血无需手术探查;
C.严重肝损伤的非手术治疗后7-10天出现低血压或者红细胞压积下降通常考虑:
i.损伤部位再出血,通常是动脉性出血。住进ICU,稳定病情。iii.血管造影确诊病因。iv.血管造影栓塞血管。v. 不要进行手术探查;
PRACTICE GUIDELINES: MANAGEMENT OF LIVER INJURIES
OBJECTIVES:
- Define situations in which non-operative management of liver injuries is safe and desirable.
- Outline a protocol for non-operative management of liver injuries.
- Outline a protocol for the operative management of liver injuries.
DEFINITIONS: Fractures of the liver: Grade I:Grade II:
Grade III:
Grade IV: Grade V:
GUIDELINES:
Capsular avulsion
Parenchymal fracture <1 cm deep Parenchymal fracture 1-3 cm deep
Subcapsular hematoma <10 cm in diameter
Peripheral penetrating wound Parenchymal fracture >3 cm deep
Subcapsular hematoma >10 cm
Central penetrating wound Lobar tissue destruction
Massive central hematoma Retrohepatic vena cava injury
Extensive bilobar disruption
1.
Indications for operative and non-operative management of liver injuries:a. Operative management of liver injuries should be considered when there is ongoing bleeding from the liver injury resulting in unstable vital signs or there is
the possibility of other injuries.
i. ii. iii. iv.
Markedly unstable patient with rapidly expanding abdomen or increasing rigidity.
Grossly positive peritoneal lavage.
Grade V liver injury on CT scan.A “swirl” pattern on CT scan suggestive of ongoing bleeding when angiography is not available in a timely fashion.
High velocity gunshot wound to the abdomen in the RUQ.
v.b. Non-operative management of active bleeding can be undertaken if:
i. ii. iii. iv.
Angiography for embolization is readily availableVital signs respond appropriately to fluid resuscitation There are no other obvious injuries in the abdomen
The trauma team is available to monitor the patient in the angiography suite.
c. Non-operative management of liver injuries can be undertaken in the otherwise stable patient.
- Liver injury diagnosed on CT scan with normalizing vital signs Grade I to IV: a) Injury not into hilum.b) Rim of blood fairly localized around liver.
- FAST positive for intraperitoneal fluid & liver injury diagnosed on CT in stable patient.
2.a.
b. c. d.
e. f.
Operative management:Transfer patient immediately to the operating room, have self-retaining retractors available (Bookwalter).
Prep from chin to mid-thigh, table to table.Generous midline incision from xiphoid to below the umbilicus.
Pack the RUQ with multiple lap pads. If bleeding is brisk or patient is hypotension,
consider the use of the aortic occluder device!!Pack the other quadrants and check the mesentery for bleeding. Assess the bleeding from the liver.
g.
h. i. j.
k.
iii. If bleeding is controllable but then worsens because of coagulopathy, then consider packing as interim definitive procedure.
When hepatic hemorrhage is controlled, explore the rest of the abdomen with particular
attention to porta hepatis, duodenum, pancreas and right colon.Drain liver if lacerations are deep and there is possibility of bile leak and fluid collection. If packs are placed, leave abdomen open with abdomen vac-pac.
If packs are placed, they should be removed in 24-48 hours. Prepare for this procedure with the availability of autotransfusion, the argon beam coagulator and blood products. If packs are placed, treat with antibiotics.
i.
If the bleeding is brisk, clamp the porta hepatis with your finger or a non-crushing clamp (Pringle maneuver).a) If bleeding persists, consider hepatic vein injury or retrohepatic caval injury.
ii.
c) If bleeding subsides but worsens because of coagulopathy, consider packing as definitive interim procedure.
If bleeding is moderate but controllable with packs:
b)
i) Consider veno-veno bypass.ii) Consider resectional debridement to get to the vena cava and the
branches of the hepatic veins.iii) Consider median sternotomy for better controliv) Consider packing (See Damage Control Guideline).
If bleeding subsides:i) Control bleeding with suture ligatures.ii) Release Pringle maneuver and control major bleeding with suture
ligatures.iii) Consider omental pack.
a)
b) c)
i) ii) iii)
Mobilize the liver:Divide falciform ligaments.Divide lateral triangular ligaments.Rotate liver medially into wound.Explore injury (but do not worsen it).Control bleeding with suture ligatures.d) Consider liver edge approximation with large
absorbable sutures (0-chomic on liver needle). e) Consider omental pack.
3.a.
b.
Non-operative management:Admit all Grade III-IV liver lacerations or those with significant blood around the liver (with normalizing vital signs) to telemetry unit. Admit those with large amounts of blood around the liver with hematocrit <32% to the ICU. All others can be admitted to the trauma floor.
4.a.
b.
c.
Pitfalls:Fever and/or jaundice – consider biloma.
i. CT scan to confirm fluid collection around liver.ii. Radionuclide biliary excretion exam to confirm active leak.iii. Percutaneous drainage.iv. Consider ERCP with stent placement and/or sphincterotomy.
UGI bleed two to four weeks after injury – consider hemobilia. i. CT scan to confirm large intrahepatic injury or clot.ii. Angiography to confirm etiology.iii. Angiographic embolization of vessel.
iv. Do not explore for hemobilia.Hypotension, drop in hematocrit seven to ten days after non-operative management of severe liver injury:i. Repeat bleed, usually arterial.ii. Admit to ICU, stabilize.iii. Angiography to confirm etiology.iv. Angiographic embolization of the vessel.
c.
After discharge:
i. ii. iii. iv.
i. ii. vi.
Transfer to regular floor. Advance diet.Hematocrit and hemoglobin daily.
Liver enzymes and bilirubin on day 2 to help rule out biloma. If bilirubin elevated, consider a HIDA scan to rule out bile leak.Bed rest 2 days. Grade I and II liver fractures may ambulate immediately.ALL Patients receive a SOLID ORGAN INJURY Card
If stable and tolerating diet:a) Grade I and II injuries: discharge on day 1-2. b) Grade III and IV injuries: discharge on day 4.
i. ii. iii.
iv. v. vi.
No school for a week.No physical education for six weeks. No major contact sports:
a) Grade I and II: for six weeks.b) Grade III, IV and V: for three months.
Return to clinic in two weeks. Avoid alcoholic beverages Instruct to return to the ED if:
a) Worsening RUQ pain b) Feverc) Jaundiced) Hematemesis
Monitor hourly vital signs until normal (e.g., pulse < 100/min) X 3. Bed rest.NPO.
i.ii.iii.iv.When hematocrit is stable and there have been no adverse hemodynamic events:
Draw serial hematocrit and hemoglobin every 6 hours until stable (within 2 %) X 2.
v. Attempt to avoid exploration at this time