新探索,新前景!白蛋白紫杉醇联合卡铂降阶梯新辅助治疗部分早期三阴性乳腺癌疗效显著
三阴性乳腺癌(TNBC)是一种侵袭性和高度异质性的实体肿瘤,目前尚未得出早期TNBC患者的最佳降阶化疗方案及疗效预测因素。近日请赵艳霞教授为我们分析了一篇发表于《CLINICAL CANCER RESEARCH》的研究,其主要对前瞻性ADAPT-TN试验中的生存结果进行了分析,并比较了两种降阶的无蒽环类新辅助方案。此外,根据mRNA、sTIL以及经典的预后因子探讨了不同生物标志物的临床相关性以及其他辅助蒽环类化疗对pCR患者的生存影响。
研究简介
三阴乳腺癌(TNBC)患者的最佳治疗方案尚不明确,但在部分患者中使用短期降阶化疗也是一种选择。以往研究已经发现几种促免疫因子可预测TNBC的疗效,但是它们对不同化疗方案的疗效预测仍然存在争议。
ADAPT-TN是一项针对早期TNBC患者(n=336)新辅助治疗的随机多中心II期临床试验。试验随机分配患者进行12周的白蛋白紫杉醇(125 mg/m2)联合吉西他滨治疗(d 1,8 q3w),或者白蛋白紫杉醇(125 mg/m2)联合卡铂治疗(d 1,8 q3w)新辅助化疗,随即手术治疗,后续未达到PCR的患者继续使用4周期表阿霉素(90 mg/m2)联合环磷酰胺(600 mg/m2 )辅助化疗,达到病理完全缓解(pCR)的患者则终止进一步化疗。研究结果主要观察无侵袭性/无远处疾病生存和总生存期(i/dDFS、OS),并通过nCounter平台和基质肿瘤浸润淋巴细胞(sTIL)测定119个基因表达(包括PAM50亚型),探索量化标志物对化疗降阶的预测影响。
研究结果发现:化疗12周能否达到pCR与5年iDFS显著相关,达到pCR与未达到pCR患者的5年iDFS分别为90.6%和62.8%(HR,0.24; P =0.001)。白蛋白紫杉醇联合卡铂组相对于联合吉西他滨组pCR率较高,但未观察到使用卡铂的生存优势(HR,1.04;95% CI,0.68–1.59)。在达到pCR患者中,额外使用蒽环类药物化疗也与iDFS的显著优势无关(HR,1.29;95% CI,0.41-4.02)。进一步发现除了pCR率之外,淋巴结状态和高sTIL与更好的iDFS和OS均独立相关。
结论:对早期TNBC患者来说,短期降阶新辅助白蛋白紫杉醇联合卡铂对部分TNBC患者是一种很有前景的策略,可将pCR率、淋巴结阴性和高sTILs作为进一步(降阶)升阶梯治疗的早期决策点。
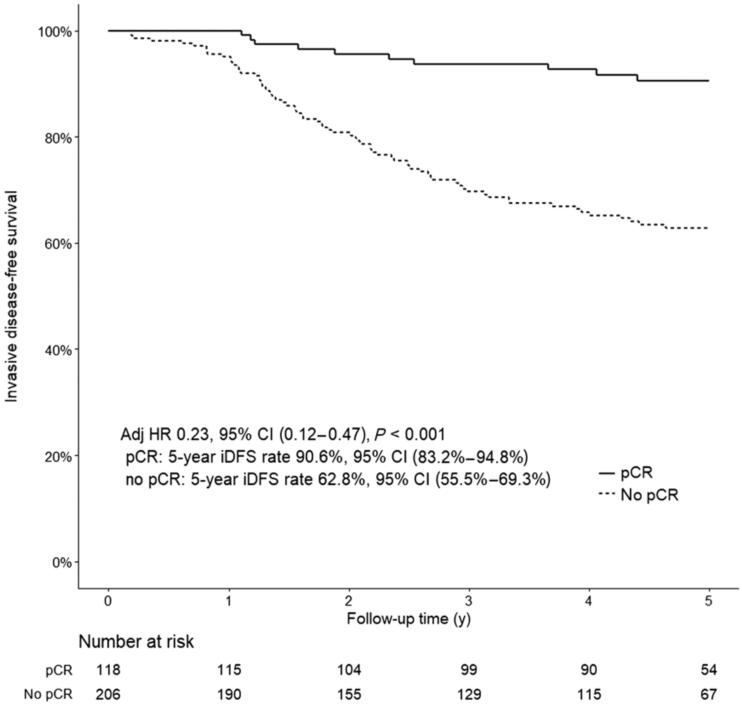
12周治疗后患者无侵袭性疾病生存率曲线
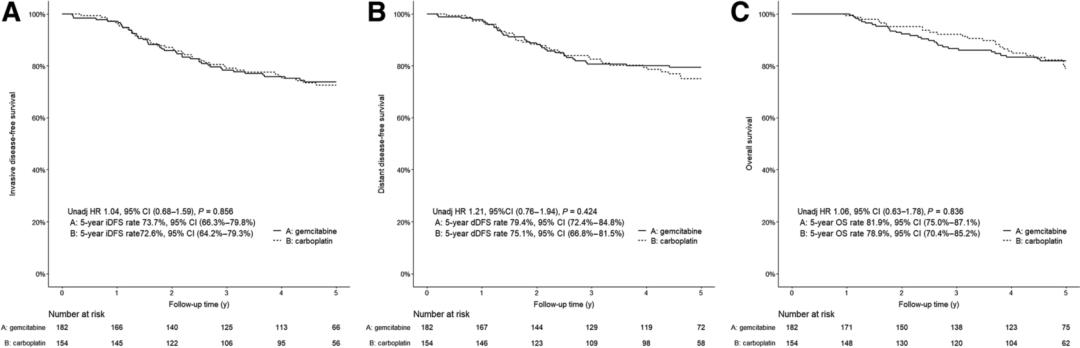
△研究中的无侵袭性疾病生存(A)、无远处疾病生存(B)和总生存率(C)
研究讨论
此项针对TNBC的新辅助化疗的研究中,短疗程白蛋白紫杉醇联合卡铂治疗在pCR率方面优于白蛋白紫杉醇联合吉西他滨治疗1。在谨慎比较不同试验结果后发现,12周治疗后pCR率与常规新辅助化疗方案类似2。这种相似性表明12周pCR有望作为(降)升阶策略的早期决策点。
本研究结果与CALBG 40603结果一致,该II期-III期临床试验通过对TNBC患者(n=443)进行中位随访5年发现,在标准蒽环类-紫杉烷-环磷酰胺联合治疗中加入卡铂并没有显著改善生存影响3。GeparSixto研究发现在非标准蒽环类-紫杉烷-贝伐单抗联合治疗中加入卡铂对TNBC患者3年DFS有显著改善4;然而与剂量密集及强化剂量的含环磷酰胺方案相比,前者与提高iDFS或者OS无关5。
相比之下,最近的一些研究表明,在TNBC患者中卡铂可能是蒽环类的最佳替代品,而不是作为蒽环联合紫杉烷治疗的补充药物6-7。ADAPT- TN试验中研究者将卡铂作为替代品,并将其与白蛋白紫杉醇联合治疗,对照组为溶剂型紫杉醇联合卡铂治疗8-10。
WSG-ADAPT-TN的生存数据证实了近期发现的sTILs高表达(而不是PD-1高表达)可作为eTNBC群体有利的预后标志物11-13。
根据本研究及其他研究结果,短期白蛋白紫杉醇紫杉卡铂联合治疗是一种有前景的NACT降阶疗法14-16。
TNBC的异质性更加需要个体化治疗理念。本项研究表明短期铂类降阶化疗方案的新辅助治疗可以安全地作为诱导治疗实施,将pCR作为进一步(降阶)升阶治疗的早期决策点。现有证据及本研究结果表明TNBC个体化治疗理念的选择标准不仅应考虑免疫学标志物(如sTILs或PD1),而且还应该考虑新辅助化疗的反应及临床风险。
鉴于在ADAPT TN试验中的eTNBC和pCR患者仅完成12周含有紫杉烷铂类方案治疗后并没有进一步进行任何化疗,而群体预后良好,显然需要在早期TNBC群体中进行进一步的降阶试验。

赵艳霞 教授
华中科技大学同济医学院附属协和医院
医学博士,主任医师,副教授,硕士生导师
武汉协和医院肿瘤中心乳腺肿瘤科II病区主任
中国临床肿瘤学会乳腺癌专家委员会委员
中国临床肿瘤学会青年专家委员会常务委员
中国抗癌协会乳腺癌专业委员会青年专家
中国医师协会肿瘤分会乳腺专委会委员
湖北省抗癌协会乳腺癌专业青年委员会副主任委员
湖北临床肿瘤学会青年专家委员会副主任委员
湖北省抗癌协会康复与姑息专家委员会常务委员
湖北省抗癌协会乳腺癌专业委员会委员
▌原文链接:
https://aacrjournals.org/clincancerres/article-abstract/doi/10.1158/1078-0432.CCR-22-0482/707292
参考文献
1 Gluz O, Nitz U, Liedtke C, Christgen M, Grischke EM, Forstbauer H, et al. Comparison of neoadjuvant Nab-paclitaxelþcarboplatin vs. Nab-paclitaxelþgemcitabine in triple-negative breast cancer: randomized WSG-ADAPTTN trial results. J Natl Cancer Inst 2018;110:628–37
2 Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet North Am Ed 2014;384:164–72
3 Shepherd JH, Ballman K, Polley M-YC, Campbell JD, Fan C, Selitsky S, et al. CALGB 40603 (Alliance): long-term outcomes and genomic correlates of response and survival after neoadjuvant chemotherapy with or without carboplatin and bevacizumab in triple-negative breast cancer. J Clin Oncol 2022;40:1323–34.
4 Loibl S, Weber KE, Timms KM, Elkin EP, Hahnen E, Fasching PA, et al. Survival analysis of carboplatin added to an anthracycline/taxane-based neoadjuvant chemotherapy and HRD score as predictor of response—final results from GeparSixto. Ann Oncol 2018;29:2341–7.
5 Schneeweiss A, M€obus V, Tesch H, Klare P, Denkert C, Kast K, et al. 160O Survival analysis of the randomized phase III GeparOcto trial comparing neoadjuvant chemotherapy (NACT) of iddEPC versus weekly paclitaxel, liposomal doxorubicin (plus carboplatin in triple-negative breast cancer, TNBC)(PM(Cb)) for patients (pts) with high-risk early breast cancer (BC). Ann Oncol 2020;31:S303–S4
6 Yu K-D, Ye F-G, He M, Fan L, Ma D, Mo M, et al. Effect of adjuvant paclitaxel and carboplatin on survival in women with triple-negative breast cancer: a phase 3 randomized clinical trial. JAMA Oncol 2020;6:1390–6.
7 Braybrooke J, Bradley R, Gray R, Hills R, Liu Z, Pan H, et al. Taxane with anthracycline versus taxane without anthracycline: an individual patient-level meta-analysis of 16,500 women with early-stage breast cancer in 13 randomised trials. Cancer Res 2022;82:GS2–06.
8 Untch M, Jackisch C, Schneeweiss A, Schmatloch S, Aktas B, Denkert C, et al. NAB-paclitaxel improves disease-free survival in early breast cancer: GBG 69– GeparSepto. J Clin Oncol 2019;37:2226–34
9 Gianni L, Mansutti M, Anton A, Martínez LC, Bisagni G, Bermejo B, et al. Eventfree survival analysis of the prospectively randomized phase III ETNA study with neoadjuvant nab-paclitaxel (nab-P) versus paclitaxel (P) followed by anthracycline regimens in women with HER2-negative high-risk breast cancer. J Clin吧Oncol 2019;37:515.
10 Untch M, Jackisch C, Schneeweiss A, Conrad B, Aktas B, Denkert C, et al. Nabpaclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto;GBG 69): a randomised, phase 3 trial. Lancet Oncol 2016;17:345–56
11 Loi S, Drubay D, Adams S, Pruneri G, Francis PA, Lacroix-Triki M, et al. Tumorinfiltrating lymphocytes and prognosis: a pooled individual patient analysis of early-stage triple-negative breast cancers. J Clin Oncol 2019;37:559–69
12 Salgado R, Denkert C, Campbell C, Savas P, Nuciforo P, Aura C, et al. Tumorinfiltrating lymphocytes and associations with pathological complete response and event-free survival in HER2-positive early-stage breast cancer treated with lapatinib and trastuzumab: a secondary analysis of the NeoALTTO TrialTILs and outcomes in HER2 breast cancer treated with Lapatinib and TrastuzumabTILs and outcomes in HER2 breast cancer treated with lapatinib and trastuzumab. JAMA Oncol 2015;1:448–55
13 Sabatier R, Finetti P, Mamessier E, Adelaide J, Chaffanet M, Ali HR, et al. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget 2014;6:5449–64.
14 Gluz O, Kolberg-Liedtke C, Prat A, Christgen M, Gebauer D, Kates R, et al. Efficacy of deescalated chemotherapy according to PAM50 subtypes, immune and proliferation genes in triple-negative early breast cancer: primary translational analysis of the WSG-ADAPT-TN trial. Int J Cancer 2020;146:262–71.
15 Schmid P, Cortes J, Pusztai L, McArthur H, Kummel S, Bergh J, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med 2020; 382:810–21.
16 Mittendorf EA, Zhang H, Barrios CH, Saji S, Jung KH, Hegg R, et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracyclinebased chemotherapy versus placebo and chemotherapy in patients with earlystage triple-negative breast cancer (IMpassion031): a randomised, double-blind,phase 3 trial. Lancet North Am Ed 2020;396:1090–100.
审批号:CN-105892
本文由阿斯利康提供支持,仅供医疗卫生专业人士参考。