Accidental Intrathecal Injection of Aminophylline in Spinal Anesthesia
腰麻意外鞘内注射氨茶碱一例报道
Muhammad Ajmal, M.B.B.S., D.A.*
Anesthesiologist, Aziz Fatima Hospital, Faisalabad, Pakistan. Current position: Resident, Department of Anesthesia, Letterkenny,General Hospital, Letterkenny, Ireland.
MEDICATION error has been an unfortunate chapter in the history of spinal anesthesia since its invention in 1899. Many catastrophic incidents have occurred from intrathecal injection of local anesthetics contaminated with other chemicals as well as the use of drugs not intended or approved for intrathecal administration.1–5 In such situations, patient outcomes depend on the nature of the contaminant or the drug effects. Outcomes range from transient neurologic symptoms to permanent neurologic damage, including paraplegia.1–5 Although there are reports on a wide variety of medication errors in spinal anesthesia,1–5 accidental intrathecal use of aminophylline, a bronchodilator, has not been described previously.
自1899年发明腰麻以来,用药错误从未断过。许多灾难性事件源于鞘内注射被其他化学物质污染的局部麻醉剂,以及使用非计划或未经批准可用于鞘内给药的药物[1-5]。在这种情况下,患者的预后取决于污染物的性质或药物作用。结局包括从短暂的神经症状到永久性神经损伤,包括截瘫[1-5]。尽管腰麻中有各种用药错误的报告[1-5],但鞘内意外使用氨茶碱(一种支气管扩张剂)尚未见报道。
Case Report
This case is reported with the consent of the patient’s next-of-kin. A healthy, 64-yr-old man (70 kg) was scheduled for transurethral prostate resection for benign hyperplasia. The night before surgery, the patient was assessed and spinal anesthesia was planned.
个案报道
该病例报道已获患者*亲近**同意许可。一名64岁健康男性(70公斤),因前列腺增生,计划行经尿道前列腺切除术。术前一晚,对患者进行评估,并计划行腰麻下手术。
Before lumbar puncture, using a 5-ml disposable syringe, the anesthesiologist drew and injected supposed 3 ml plain bupivacaine (bupicain), 0.5%, from a single-use 10-ml amber-colored glass ampoule held by an assistant. Using aseptic technique, with the patient in a seated position, lumbar puncture was successful on first attempt at L3–L4 with a 23-gauge cutting spinal needle.
腰麻穿刺前,麻醉医生先用5毫升一次性注射器,从助手拿的一次性10毫升琥珀色玻璃安瓿中抽取3毫升的“0.5%布比卡因”。然后,患者坐姿,采用无菌技术,用23号腰麻穿刺针在L3–L4棘突间隙进行穿刺,一次成功,再注射抽取的3毫升“0.5%布比卡因”。
Immediately after intrathecal injection, the patient’s lower limbs (calves) developed tetanic muscle spasm and he complained of leg cramping. This unusual response aroused suspicion. After closer inspection, it was determined that aminophylline had been injected intrathecally instead of bupivacaine. The size, shape, and color of the 10-ml aminophylline ampoule (GlaxoSmithKline [formerly known as Wellcome], Karachi, Pakistan) was similar to that of the 10-ml bupicain ampoule (Howard, Lahore, Pakistan; fig. 1).
鞘内注射后,患者下肢(小腿后部)立即出现强直性肌肉痉挛,腿抽筋。此异常反应引起怀疑。仔细检查后,确定鞘内注射的是氨茶碱而不是布比卡因。10毫升氨茶碱安瓿(巴基斯坦卡拉奇葛兰素史克生产,前身为Wellcome)的大小、形状和颜色与10毫升布比卡因安瓿相似(巴基斯坦拉合尔霍华德生产,图1)。

Fig. 1. Ten milliliter ampoules of bupivacaine (bupicain), 0.5%, versus aminophylline: similar size, shape, and color.
图1. 10毫升0.5%布比卡因安瓿和氨茶碱安瓿外观:大小、形状和颜色相似。
General anesthesia was induced immediately with 400 mg sodium thiopental and 100 mg suxamethonium. Tracheal intubation was achieved using an 8-mm ID cuffed endotracheal tube. Anesthesia was maintained with nitrous oxide, oxygen, and halothane mixture. Atracurium besilate was used to facilitate controlled ventilation.
立即用400mg硫喷妥钠和100mg琥珀胆碱诱导,用内径8mm的袖套式气管插管,进行全身麻醉。用氧化亚氮、氧气和氟烷混合物维持麻醉。用苯磺酸阿曲库铵肌松,改善控制性通气。
The patient remained stable during surgery, which lasted 45 min. Intravenous dexamethasone (8 mg) was injected during anesthesia. Surgical management was customary for transurethral resection of prostate.
继续手术,术式为常规经尿道前列腺电切术。术中患者保持稳定,手术时间45分钟。麻醉期间静脉注射地塞米松(8 mg)。
After recovery from anesthesia, the patient was comfortable and results of the neurologic examination were normal. Although the literature was searched to acquire any information regarding similar medication errors, no such report was available.6 Immediately after the error and for the duration of the patient’s hospital stay (24 h), he remained in normal condition. He did not exhibit neurologic problems or any other complaints.
麻醉苏醒后,患者未感异常,神经系统检查结果正常。查文献寻找有无类似用药错误,但没有此类报告[6]。错误发生即刻以及住院期间(24小时),患者状态正常。未见有明确的神经损伤表现或任何其他症状。
In the absence of any clinical signs or symptoms of distress, and in the absence of any clinically proven intrathecal intervention(e.g., intrathecal lavage to mitigate the effects of aminophylline medication error), a “wait and see” policy was followed.7 The patient was, therefore, discharged from the hospital.
因无异常临床症状或体征,也未进行任何临床证明的鞘内干预(例如,鞘内灌洗以减轻氨茶碱用药错误影响),患者出院,继续观察[7]。
The patient reported back to the hospital within 24 h of release because of weakness in his lower limbs. His care was transferred to a medical specialist who treated him with a high dose of vitamin B-complex oral supplements. Although it was hoped that the supplements would revitalize damaged neurons, no such treatment proved fruitful. Three days after the incident, a lumbar puncture was done to obtain cerebrospinal fluid specimen and to perform a myelogram. Results of cerebrospinal fluid analysis were considered normal, with elevated protein concentrations (54 mg/dl [normal=15–45 mg/dl]). Lateral and oblique views of the lumbar myelogram showed mild external compression on the thecal sac at L3–L5, most likely the result of disc bulging at those levels. However, this type of radiographic finding is common in significant proportion within a healthy, asymptomatic population. Vertebral heights and disc spaces were likewise normal (fig. 2).
因为下肢无力,患者出院后24小时内又返回医院。请另一医学专家会诊,给予大剂量复合维生素B口服治疗,希望能有效治疗受损神经元,结果无效。三天后,行腰椎穿刺以获取脑脊液并进行脊髓造影。脑脊液分析结果正常,但蛋白质浓度升高(54毫克/分升[正常=15–45毫克/分升])。腰椎侧位和斜位脊髓造影显示L3–L5处硬膜囊轻微受压,很可能系由该部位椎间盘膨出所致。然而,在大部分健康、无症状的人群中,这种轻微受压很常见。椎体和椎间隙高度均正常(图2)。
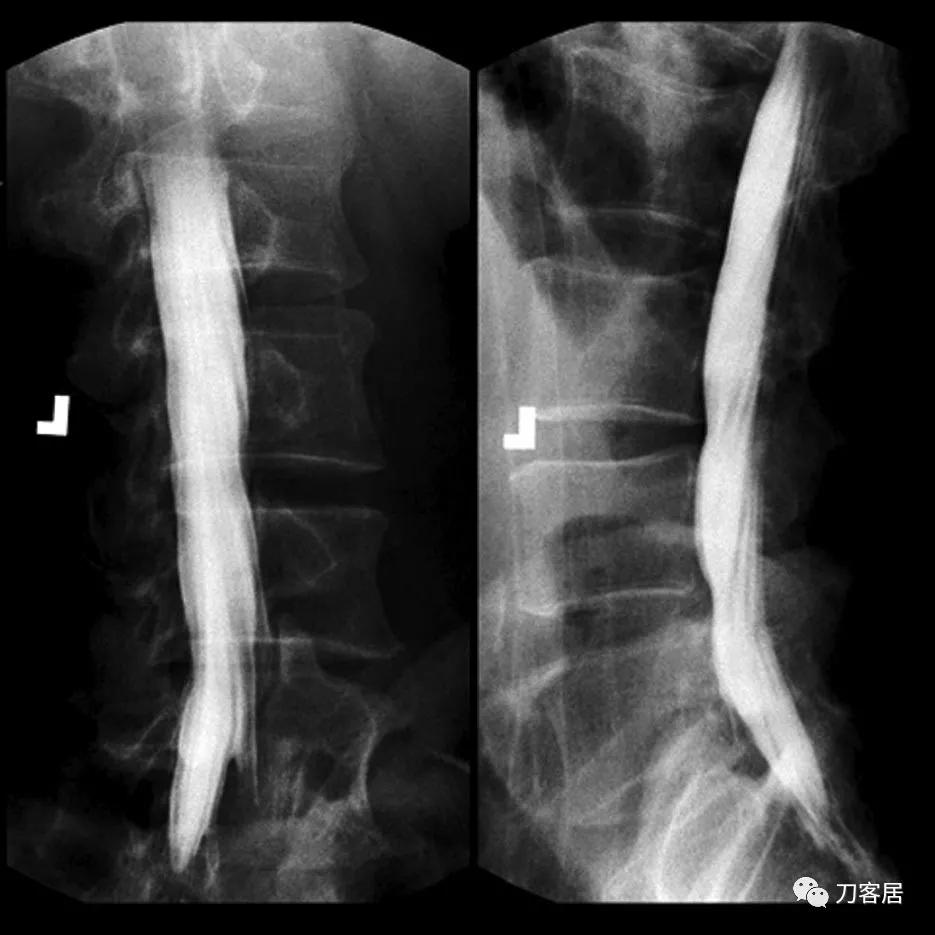
Fig. 2. Lumbar myelogram taken on third day after medication error. In preparation for transurethral prostate resection for benign hyperplasia, an intrathecal injection of 3 ml aminophylline was administered instead of bupivacaine (bupicain), 0.5%.
图2。用药错误后第三天进行腰椎脊髓造影。在准备经尿道前列腺电切术治疗前列腺增生时,误将3毫升氨茶碱当作0.5%布比卡因进行鞘内注射。
Medical professionals involved in case management were convinced that no measure at that stage could modify the outcome. Advanced imaging technology, such as magnetic resonance imaging, was not freely available--nor was the patient willing to bear the expense of further investigation that could not modify the outcome. Although pathologic diagnosis remained obscure, clinical diagnosis of the case was obvious: 3 ml aminophylline, 2.5%, had done the damage. The patient remained paraplegic and died 2 yr later. Considering social background and medical history, no autopsy was performed.
参与该病例处理的医疗专业人员确信,现阶段已无任何有效措施可以改变结果。没有先进影像检查,如磁共振,患者也不愿意再做不能改变结果的进一步检查。虽然病理诊断仍不明确,但该病例的临床诊断明确: 3毫升2.5%的氨茶碱造成神经损害,病人截瘫,2年后死亡 。考虑到社会背景和病史,没有进行尸检。
Drugs administered inadvertently during central neuraxial blocks have resulted in serious consequences as a result of direct drug or drug-additive neurotoxicity as well as extreme pH of the injectate. Pain on intrathecal injection is the most common sign when an irritant solution such as a local anesthetic is contaminated with an acid or antiseptic solution.8
由于药物或药物添加剂的神经毒性以及注射液的极端pH值,腰麻时药物误用已导致严重后果。当刺激性溶液(如局部麻醉剂)被酸或抗菌/防腐剂溶液污染时,鞘内注射后疼痛是最常见的症状[8]。
The patient described in this report did not complain of pain on intrathecal injection of aminophylline- even though it was a strong alkaline solution composed of theophylline and ethylenediamine (4:1). Theophylline is a methylxanthine and nonspecific phosphodiesterase inhibitor. It is central nervous system stimulant when used systemically and can lead to convulsions with toxic plasma levels. Its inadvertent intrathecal injection in the reported case resulted in initial excitation of spinal neurons. In some animal models, intrathecal aminophylline was shown to block the locus coeruleus stimulation-mediated antinociception in parafascicular neurons by antagonizing the adenosine receptors.9 Ethylenediamine forms a stable mixture with theophylline to produce aminophylline. It is widely used in the chemical and pharmaceutical industries. Headache, dizziness, shortness of breath, nausea, and vomiting have been reported after exposure. It irritates the skin and mucous membranes. In the form of aminophylline, ethylenediamine is a diluted solution. It can cause skin burns in concentrated form. Allergic skin reactions can occur in individuals sensitized to this chemical.10
尽管氨茶碱为茶碱和乙二胺(4:1)组成的强碱溶液,但该病例鞘内注射氨茶碱没有引起疼痛。茶碱是一种甲基黄嘌呤和非特异性磷酸二酯酶*制剂抑**,全身使用时,对中枢神经系统有兴奋作用,达到一定血浆毒性浓度后可导致抽搐。该病例中,意外鞘内注射导致脊髓神经元兴奋。在一些动物模型中,鞘内注射氨茶碱可通过拮抗腺苷受体阻断刺激蓝斑介导的椎体束旁神经元抗伤害作用[9]。乙二胺与茶碱稳定结合形成氨茶碱,广泛应用于化工和制药行业。据报道,接触后可出现头痛、头晕、呼吸短促、恶心和呕吐。它可刺激皮肤和粘膜。以氨茶碱形式存在的乙二胺,是一种稀释溶液,高浓度时可导致皮肤烧伤,对此化学药品敏感的个体,可导致过敏性皮肤反应[10]。
In Pakistan, the country where this incidence occurred, supply of consumable items (e.g., medications, needles, canulae, sutures, etc.) required for anesthesia or surgery has been the responsibility of patients. They or their family members are required to purchase the necessary items from various medical stores or pharmacies and deliver them to operating rooms before, during, and after surgery, as needed. Operating departments cannot ensure uniformity in drug supplies, increasing the risk of medication errors.
在巴基斯坦, 发生这种情况的国家,麻醉或手术所需耗材(如药物、针头、套管、缝线等)一直由患者自行准备。患者或其家庭成员根据需要从各种医疗商店或药店购买后在手术前、手术中和手术后送到手术室。手术室无法保证药品供应的一致性,增加了药品误用风险。
After a medication error of this kind has occurred, often there is no definitive treatment strategy available. Prevention of such errors is the only measure to ensure patient safety. Strategies such as clear labeling and a system to ensure accurate drug identification are essential components of such preventive programs.7,11Ultimately, it is the anesthesiologist who is responsible and answerable for the safety of his or her patients.
发生此类药物错误后,通常没有明确的治疗策略可用。预防此类错误是确保患者安全的唯一措施。标签清晰和正确药物识别是此类预防系统策略中的重要组成部分[7,11]。最终,麻醉医生应对其患者的安全负责。
参考文献:略