第三篇
万古霉素最新指南要点分析和临床知识点延伸
作者
Jingyi Wang, PharmD, University of Cincinnati, College of Pharmacy
Yutong Yang, PharmD candidate, University of Washington, School of Pharmacy
Christine Dai, PharmD candidate, University of Washington, School of Pharmacy
Tracy Zhang, PharmD candidate, The Ohio State University, College of Pharmacy
审核
Zhen Zhang, PharmD, BCPS, RPCCC
翻译
林琳 华侨大学医学院
杜青青 重庆医科大学附属第二医院
第一篇链接:
The new vancomycin guideline and elaborating pearls -- Part I
万古霉素最新指南要点分析和临床知识点延伸 -- 第一篇
第二篇链接:
The new vancomycin guideline and elaborating pearls -- Part II
万古霉素最新指南要点分析和临床知识点延伸 -- 第二篇
原文 :
The new vancomycin guideline and elaborating pearls -- Part III
05 AUC指导的剂量调整
vanco
Bayesian法估算的用药剂量策略
Bayesian法指导给药是万古霉素监测的最佳方法,它依赖于Bayesian剂量优化软件程序,该程序现已容易获得,可用于实时识别最佳的万古霉素剂量,以达到AUC目标。
Bayesian剂量优化软件嵌入了基于丰富采样的万古霉素数据的PK模型,称为Bayesian先验。只需收集患者用药后最初24-48小时内的万古霉素血药浓度,无需稳态浓度,该软件即可计算Bayesian后验参数值分布,并提供包括前载剂量在内的最佳给药方案。
也可以将患者的CrCl纳入PK模型,以提供更具患者个体针对性的方案,其在重症患者中非常有用。
一级动力学方程
一级动力学方程可以用作替代 Bayesian 软件的方法,对万古霉素进行监测和剂量调整。此方法需要两个稳态时的血清万古霉素浓度(C1、C2)。理想情况下,在完成万古霉素输注后的1-2小时获得C1;在下个剂量给药前测C2,接近谷浓度(Ctrough)。
这里我们提供了两种使用一级动力学方程估算AUC的方法:
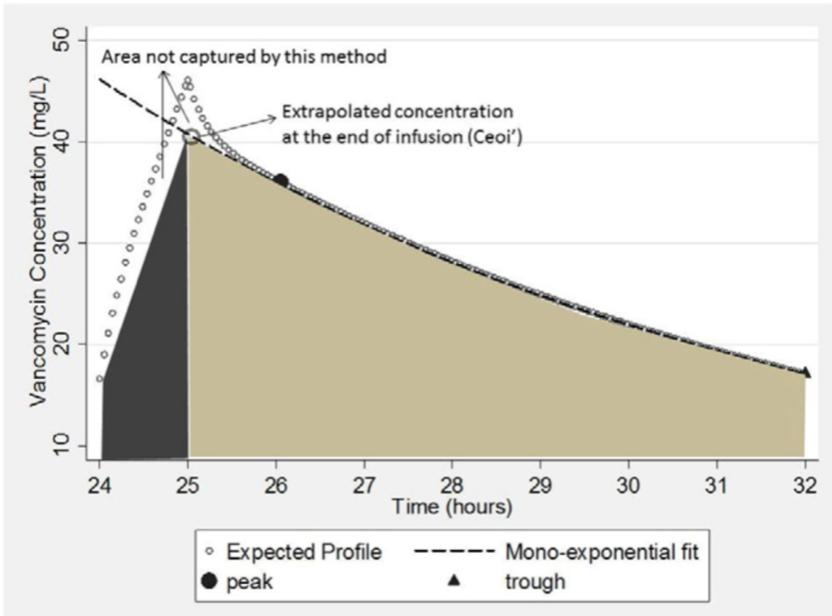
🔺方法 1 (Pai, 2014) [12]:

🔱 标注:输液时间为t’,在t1时获得C1,t2时获得C2,推算输注结束时的浓度为 Ceoi’
使用此方法计算AUC时,AUC估值偏低,如下图所示:
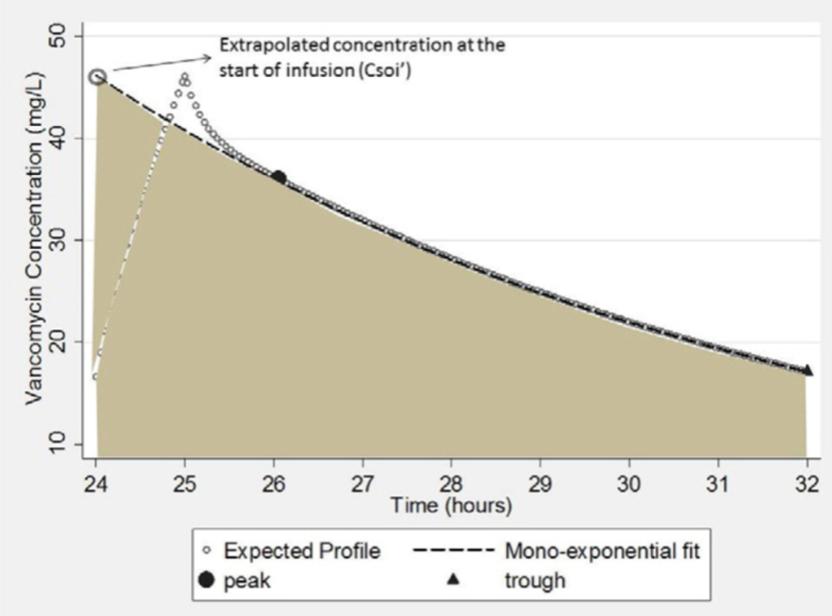
🔺方法 2 (Pai, 2014) [12]:

🔱 标注:推算输注开始时的浓度 Csoi’
使用此方法计算AUC时,AUC的估值偏高,如下图所示
❗如果每日多次给药万古霉素,则需将每次给药后的AUC与给药频率相乘,计算24小时AUC值。
实用方程:
💠 计算Ke(消除速率常数)
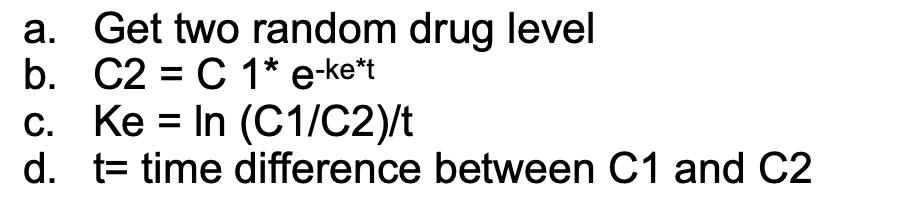
💠 如果上述两个随机药物浓度不在波峰和波谷水平,请找到患者的峰浓度 Cpeak 和谷浓度 Cmin。对于万古霉素,Cpeak是给药后一小时对应的浓度,Cmin为给药前半小时对应的浓度。

💠 计算Vd(表观分布容积)
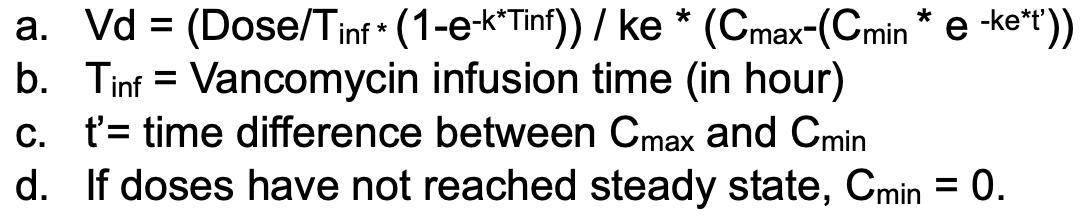

使用一级动力学方程最大的缺点就是,它仅在采样周期内提供AUC的时间点值。如果万古霉素尚未达到稳态或者患者的情况不稳定,则估计的AUC可能不准确。
采样时间
为达到最佳临床效果,目标AUC值应尽早达到,最好是在用药最初的24至48小时内。
监测频率应根据临床判断:对于血流动力学不稳定的患者,应频繁或每日进行监测;对于血流动力学稳定的患者,监测可以延长到每周一次。
临床精要
万古霉素的敏感性
〽假设万古霉素的MIC为1 mg/L
〽即使MIC<1 mg/L,也不推荐减少剂量
〽重要的是,在重症患者中最好通过BMD法验证MIC。当MICBMD>1 mg/L时,使用常规剂量达到目标AUC/MIC≥400的可能性较低。
根据最近的国内外研究,MRSA对万古霉素的敏感性一直保持不变,超过90%的分离株的MIC≤1 mg/L,且在未来的20年中潜变的可能性较小。因此,在监测中将MIC设定为1 mg/L。
MIC的测量方法共有5种,包括:BD Phoenix法、MicroScan Walk Away法、Vitek 2法、Etest法及BMD法。由于上述5种方法中MIC的结果差异大,即使MIC显示<1 mg/L,也不建议减少给药剂量。
在感染MRSA的重症患者中,必须通过标准化方法(最好是BMD法)验证MIC。Etest法可能会产生比BMD法高1.5-2倍的稀释值,所以400-600的 AUC/MICBMD 比值相当于200-400的 AUC/MICEtest 比值。
见
第
四 条
References
1. Men, Peng, et al. “Association between the AUC0-24/MIC Ratio of Vancomycin and Its Clinical Effectiveness: A Systematic Review and Meta-Analysis.” PloS One., vol. 11, no. 1, 2016, p. E0146224.
2. Michael Rybak, Pharm.D., M.P.H., Ben Lomaestro, Pharm.D., John C. Rotschafer, Pharm.D., Robert Moellering, Jr., M.D., William Craig, M.D., Marianne Billeter, Pharm.D., BCPS, Joseph R. Dalovisio, M.D., Donald P. Levine, M.D., Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists, American Journal of Health-System Pharmacy, Volume 66, Issue 1, 1 January 2009, Pages 82–98, https://doi-org.offcampus.lib.washington.edu/10.2146/ajhp080434
3. Del Mar Fernández de Gatta Garcia M Revilla N Calvo MV et al. . Pharmacokinetic/pharmacodynamic analysis of vancomycin in ICU patients. Intensive Care Med. 2006; 33:279–85.
4. Adane, Eyob D, et al. “Pharmacokinetics of Vancomycin in Extremely Obese Patients with Suspected or Confirmed Staphylococcus Aureus Infections.” Pharmacotherapy : Official Journal of the American College of Clinical Pharmacy., vol. 35, no. 2, pp. 127–139.
5. Young, Tramaine, et al. “Methodological Study of Vancomycin Dosing in Elderly Patients Using Actual Serum Creatinine Versus Rounded Serum Creatinine.” Drugs in R & D., vol. 17, no. 3, pp. 435–440.
6. Garcia L. 2010. Broth Microdilution MIC Test, p 25-41. In Clinical Microbiology Procedures Handbook, 3rd Edition. ASM Press, Washington, DC. doi: 10.1128/9781555817435.ch5.2
7. Rowena Jenkins, Sarah Maddocks, in Bacteriology Methods for the Study of Infectious Diseases, 2019
8. Rybak, Michael J, et al. “Evaluation of Vancomycin Susceptibility Testing for Methicillin-Resistant Staphylococcus Aureus: Comparison of Etest and Three Automated Testing Methods.” Journal of Clinical Microbiology : JCM., vol. 51, no. 7, pp. 2077–2081.
9. S. J. van Hal, T. P. Lodise, D. L. Paterson, The Clinical Significance of Vancomycin Minimum Inhibitory Concentration in Staphylococcus aureusInfections: A Systematic Review and Meta-analysis, Clinical Infectious Diseases, Volume 54, Issue 6, 15 March 2012, Pages 755–771, https://doi.org/10.1093/cid/cir935
10. Hale, Cory M, et al. “Are Vancomycin Trough Concentrations of 15 to 20 Mg/L Associated With Increased Attainment of an AUC/MIC ≥ 400 in Patients With Presumed MRSA Infection?” Journal of Pharmacy Practice., vol. 30, no. 3, pp. 329–335.
11. Patel N, Pai MP, Rodvold KA, Lomaestro B, Drusano GL, Lodise TP. Vancomycin: we can’t get there from here. Clin Infect Dis. 2011; 52(8):969-974.
12. Pai MP, Neely M, Rodvold KA, Lodise TP. Innovative approaches to optimizing the delivery of vancomycin in individual patients. Adv Drug Deliv Rev. 2014; 77:50-57.